Introduction
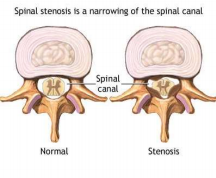
Spinal stenosis is a narrowing of one or more areas in your spine — most often in your neck or lower back.
How does spinal stenosis develop?
Primary congenital stenosis is relatively uncommon and is present at birth. But most people have acquired spinal stenosis, which develops later in life, usually as a result of degenerative and age related changes in the spine.
Between the vertebrae (bones) are intervertebral discs (connective spongy tissue like a cushion) which wear down and lose water content with age. This can result in reduced disc height and may also lead to bulging into the spinal canal. The facet joints, bones and ligaments can thicken and enlarge, due to arthritis. In an attempt to repair the damage, the body may produce bony growths called bone spurs. All the above can lead to narrowing of spinal canals causing stenosis. Spinal Stenosis can further lead to a number of problems, depending on spinal cord or nerve root involvement.
Signs and symptoms:
Spinal narrowing doesn’t always cause problems. But if the narrowed areas compress the spinal cord, spinal nerves or circulation of the spine,it may lead to developing signs and symptoms. These often start gradually and may get worse over time. Common pain may be episodic (on & off), recurrent and may vary in severity.
The most common symptoms include:
Pain/cramping/fatigue/numbness in the back & legs on walking and standing.
⮚ Pain in the neck & shoulders/arms.
⮚ Bending forward or sitting may reduce pain.
⮚ Weakness in legs and arms with less use of hands.
⮚ Severe neck related stenosis may cause balance disturbances while walking.
⮚ Rarely loss of bowel or bladder function may occur.
Screening and diagnosis
To help diagnose spinal stenosis and rule out other disorders, your doctor will ask about your medical history and perform a physical exam that may include checking your peripheral pulses, range of motion, and leg reflexes.
You are also likely to have one or more of the following tests:
⮚ Spinal X-ray weight bearing
⮚ Magnetic resonance imaging (MRI)..
⮚ Computerized tomography (CT)
⮚ CT Myelogram.
⮚ Bone scan.
⮚ Laboratory testing
These studies can provide information about the presence, location and extent of spinal canal narrowing and nerve root involvement.
Treatment: Most people with spinal stenosis can be effectively treated with non surgical treatments.
Medications:
Our approach in spine care is to treat the condition with little or no use of oral medication that may have side effects and promote drug dependency. NSAIDs (anti-inflammatory medications to reduce swelling or inflammation), analgesics (medications to control pain), and other pain medication such as narcotic analgesics are used temporarily until we can treat the source of the pain. Long-standing use of prescription needs to be closely monitored for the development of potential problems.
Physical Therapy & Therapeutic Exercises:
Targeted Physical Therapy includes therapeutic exercises to alleviate pressure on the nerve and prevent worsening symptoms, reduce pain, improve range of motion and strengthen spine stabilizing muscles. These exercises are specific to the patient and condition, as nonspecific gym exercises may worsen this condition. Therapeutic exercises are done in stages, initial stages include goals for pain relief (gentle stretches & exercises to reduce leg pain – centralization with modalities like heat, electrical, TENS) and later stages would include more active exercises to improve flexibility, core stabilization, gym training, and endurance exercises. Emphasis is always placed on body mechanics (how you move), posture, ergonomics (work conditions), home exercises, and lifestyle changes. Weight loss, cessation of smoking and improving overall fitness and conditioning are essential in the recovery and prevention of recurrence of spine pain.
Interventional Pain Management: * Epidural steroid injections:
Epidural steroid injections may be necessary in severe cases or after physical therapy and medications have failed to provide appropriate pain relief. These injections are done at our practice under fluoroscopic (x-ray guidance) using advanced techniques in Interventional Pain Management (discussed more in another pamphlet). Potent steroids are placed at the interface of the pain source to help reduce pain and inflammation around the nerve and disc that is causing the pain in the back and to travel down the buttock or leg. It can therefore give the body a chance to heal and recover from the condition, continue with further rehabilitation and avoid surgery. It is our practice to treat pain aggressively and early (3-6months of pain onset) to try to get to the source of pain rather than masking the pain with narcotic medications or prolonged physical therapy. This is important in avoiding chronic pain, disability, disuse, dependency on drugs & emotional anxiety, and depression related to pain.
Facet Joint Blocks:
The facet joints can be a source of midline back pain when they become arthritic and inflamed, a steroid injection or nerve block reduces the inflammation and/or swelling of tissue in the joint. If facet joint and nerve (nerve supply to facet joint – Medial Branch) blocks have a positive response – Radio Frequency Neurolysis (RFN) may be indicated.
RFN is a procedure using a specialized machine to interrupt nerve conduction and reduce pain on a semi-permanent basis. The nerves can be usually blocked for 6-9 months (can be as short as 3 months or as long as 18 months) Most interventions are done in combination with comprehensive physical rehabilitation and lifestyle(weight loss, smoking cessation, etc.) modification program.
*Surgery: Surgery is not performed at our practice, however if indicated we will refer you to a qualified surgeon. If your main symptom is leg pain rather than mostly back pain, you may expect better results from surgery. Surgery may be recommended for small percentage patients who develop progressive weakness in limb muscles or bladder and bowel disturbances (Cauda Equina Syndrome). The surgery is done to open the bony canal to provide available space for the nerves called lumbar decompression surgery or laminectomy. If the vertebral bones are slipping (spondylolisthesis) or have instability (abnormal motion of vertebrae) they may require a fusion. Post Fusion rehabilitation may require up to 6 -9 months for complete return to baseline activities.