
DISC HERNIATION / SCIATICA
A herniated disc is also known as a ruptured or protruded disc. Majority of people with this condition will recover and return to their normal lifestyle without having to get surgery.
WHAT IS A HERNIATED DISC?
The lower back bone called the lumbar spine is made up of bones called vertebrae that stack up one on top of the other. In between the vertebrae is cartilage called a disc that acts like a cushion and allows your spine to bend in different direction. The disc has layers, like an onion, called the annulus fibrosus and a gel-like center called the nucleus pulposus. The disc also contains high content of water.
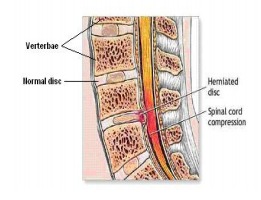
With age, the water content in the disc reduces and loses its ability to act like a cushion. This may predispose a displacement of the disc’s center (called a herniated or ruptured disc) through a crack in the outer layer.
CAUSES
Most common causes are repetitive injuries, micro or major trauma, heavy lifting, pushing, pulling activities and degenerative changes to the disc annulus.
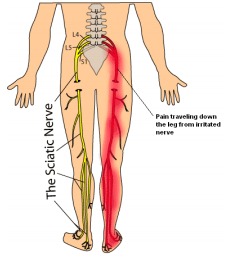
A herniated lumbar disc may also cause back pain which can travel down the leg, although back pain alone (without leg pain) can have many causes other than a herniated disc.
RISK FACTORS
Smoking, age (30-55), height (taller), sex (males) heavy work are associated with increased risk.
SIGNS AND SYMPTOMS
When a disc herniates it can irritate, inflame or compress a nerve (pinched nerve) that causes mostly pain, and sometimes numbness, tingling or weakness in the back that travels down the legs, known as sciatica which can also be associated with pain in the legs.
SCREENING & DIAGNOSING
A complete history and physical with laboratory testing is done which can identify the diagnosis, causes and future treatment options. Back or neck pain & or Sciatica can have many other causes of pain other than herniated disc.
An X-ray, CTscan and/or MRI of the lumbar spine may be indicated. A detailed MRI is most accurate in evaluating herniated discs. Often an MRI may not be indicated if symptoms are mild and active treatment can resolve symptoms. If symptoms of nerve root involvement are present for over six weeks an Electromyogram (EMG) and Nerve conduction study (NCS) can be performed. It involves using electric stimulation of nerves & a tiny needle electrode in the resting and contracting muscles supplied by affected nerves. This test can determine extent & level of actual nerve damage.
WHAT TREATMENTS ARE AVAILABLE?
Most (80-90%) patients with a new or recent acute disc herniation will improve without surgery. Treatment of this includes:
Physical Therapy: Targeted Physical Therapy includes therapeutic exercises to alleviate pressure on the nerve and prevent worsening symptoms, reduce pain, improve range of motion and strengthen spine stabilizing muscles. These exercises are specific to the patient and condition, as nonspecific gym exercises may worsen this condition. Therapeutic exercises are done in stages, initial stages include goals for pain relief (gentle stretches & exercises to reduce leg pain – centralization with modalities like heat, electrical, TENS) and later stages would include more active exercises to improve flexibility, core stabilization, gym training, and endurance exercises. Emphasis is placed on body mechanics (how you move), posture, ergonomics, home exercises, and lifestyle changes. Weight loss, cessation of smoking, and improving overall fitness and conditioning are essential in the recovery and recurrence of future episodes of spine pain.
Medications: Our approach in spine care is to treat the condition with little or no use of oral medication that may have side effects and promote drug dependency. NSAIDs, analgesics, and other pain medication are used temporarily until we can treat the source of the pain.
Trigger Point Injections: These are local injections that can control pain using anesthetics and diluted corticosteroids injected directly at the painful soft tissues or muscles along the spine or back.
Epidural steroid injections: As a herniated disc may leak chemicals or irritate the nerves, epidural steroid injections may be necessary in severe cases or after physical therapy and medications have failed to provide pain relief. These injections (discussed on another pamphlet) are done at our practice using fluoroscopic (x-ray guidance) using advanced techniques in Interventional pain management (discussed more on another pamphlet). Potent steroids are placed at the interface of the pain source to help reduce pain and inflammation around the nerve and disc that is causing the pain in the back and to travel down the buttock or leg. It can therefore give the body a chance to heal and recover from the condition, continue with further rehabilitation and avoid surgery. It is our practice to treat pain aggressively and early (3-6 months of pain onset) to try to get to the source of pain rather than masking the pain with narcotic medications or prolonged passive physical therapy. This is important in avoiding chronic pain, disability, disuse, dependency on drugs and emotional anxiety/depression related to pain.
Surgery may be indicated on an emergency basis (see below) and for certain select patients who do not respond to non-surgical treatments.
HOW DO I KNOW IF I NEED EMERGENCY SURGERY?
Rarely, a disc herniation can press on the nerves which may cause a progressive paralysis of muscles in the limbs or the nerves that control the bowel and bladder. This can be accompanied by numbness and tingling in the area around the anus or genital area & loss of bladder/bowel control – Cauda Equina Syndrome and is one of the indications for immediate surgery. Call and see a doctor immediately, if you suffer or develop any of the above symptoms. Surgery is not performed at our practice, however, if indicated we will refer you to a qualified surgeon. If your main symptom is leg pain rather than back pain, you may expect better results from surgery. Common surgeries include Discectomy or Partial Discectomy. Bone removal may be minimal or extensive – Laminectomy.